The landscape of critical care medicine has undergone a profound transformation over the past seven decades. At the forefront of this medical revolution stands Extracorporeal Membrane Oxygenation (ECMO), a life-saving technology that has evolved from experimental origins into a cornerstone of modern intensive care. As healthcare systems across the Middle East and Africa continue to advance, the integration of cutting-edge ECMO systems represents a critical leap forward in patient outcomes and survival rates.
CeroNova, as the regional distributor for Lifemotion® ECMO systems, is committed to bringing these world-class therapies closer to the patients who need them most. This article traces the chronological journey of ECMO technology, explores its current applications in critical care, and highlights how the next generation of ECMO devices is reshaping the future of medicine.
Transform your hospital’s critical care capabilities.
Contact the
CeroNova team
today to schedule a consultation and discover how the Lifemotion® ECMO system can elevate your standard of patient care.
1950s–1970s: The Dawn of Extracorporeal Support
The conceptual foundation of ECMO began in the mid-20th century with the quest to support patients during complex cardiac surgeries. The pivotal breakthrough occurred on May 6, 1953, when Dr. John H. Gibbon Jr. successfully utilized the first mechanical heart-lung machine during an open-heart operation [1]. This monumental achievement proved that a machine could temporarily assume the functions of the human heart and lungs.
However, these early cardiopulmonary bypass machines were designed for short-term surgical use, typically lasting only a few hours. The transition from intraoperative support to prolonged intensive care application required significant technological advancements. In 1971, the medical community witnessed the first successful prolonged use of ECMO in an adult patient suffering from severe lung dysfunction following a motorcycle accident [2].
Shortly after, in 1972, Dr. Robert Bartlett and his associates successfully employed cardiac ECMO for 36 hours in a two-year-old infant experiencing cardiac failure [3]. Dr. Bartlett’s subsequent success with neonates in 1976 firmly established ECMO as a viable, life-saving intervention for patients with reversible, yet severe, cardiopulmonary failure.
1980s–2000s: Standardization and the ELSO Registry
As ECMO utilization slowly expanded, the need for standardized protocols and comprehensive data collection became apparent. In 1989, the Extracorporeal Life Support Organization (ELSO) was founded [4]. This international consortium created a registry that would become the definitive source of data on ECMO outcomes, guiding clinical practice and technological refinement for decades to come.
During this era, the technology itself saw incremental improvements. Hollow-fiber oxygenators replaced older silicone membrane models, reducing complications such as plasma leakage and improving gas exchange efficiency. Despite these advancements, ECMO remained a highly specialized therapy, primarily utilized in major academic medical centers for neonatal respiratory failure, where it demonstrated remarkable success rates.
2009–2022: Pandemics and Global Expansion
The trajectory of ECMO utilization shifted dramatically during the 2009 H1N1 influenza pandemic. The publication of the CESAR trial during this period demonstrated improved survival without severe disability for adult patients with severe acute respiratory distress syndrome (ARDS) who were referred to an ECMO center [5]. This marked a turning point, expanding ECMO’s application significantly within the adult population.
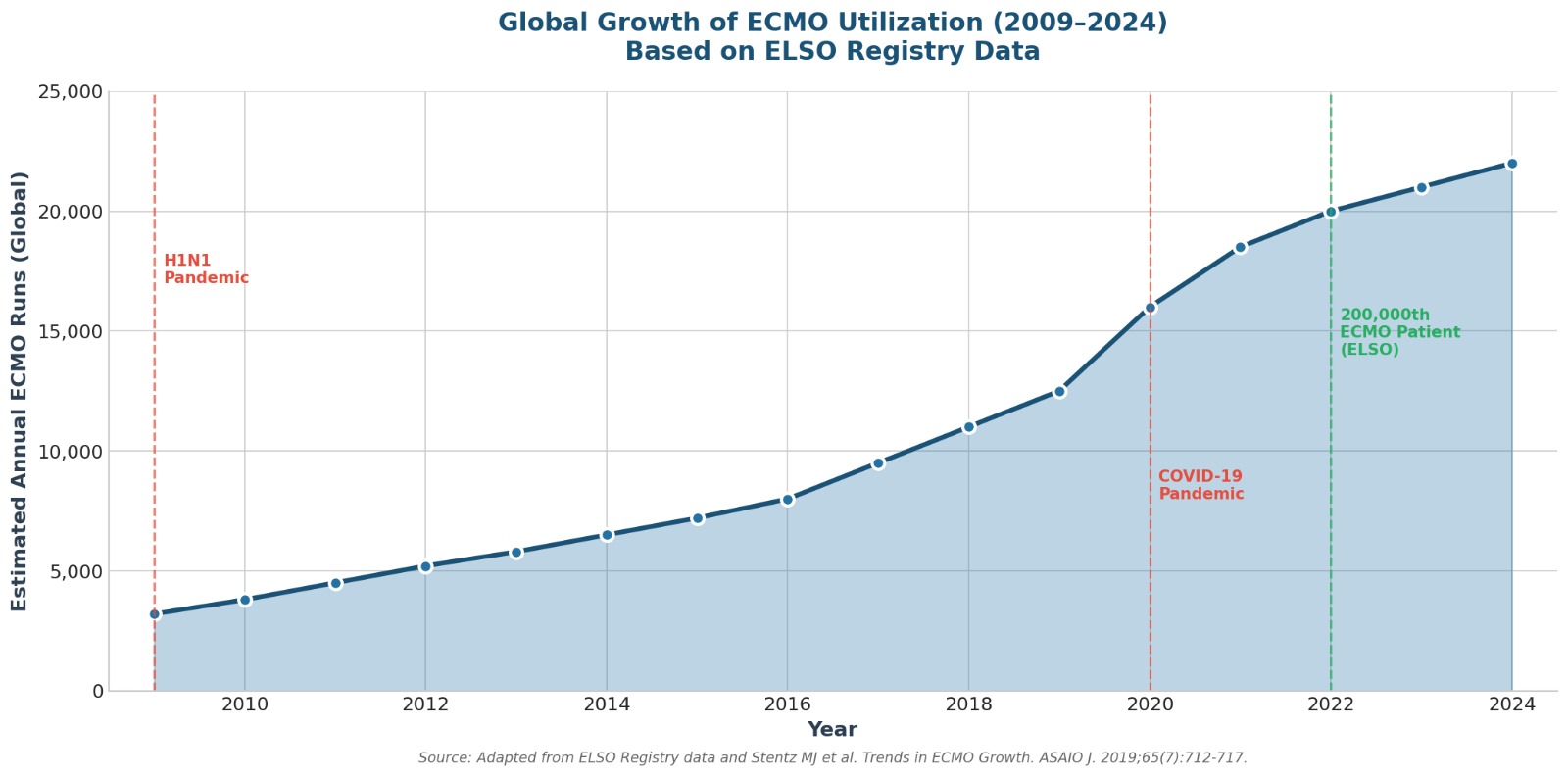
The most profound catalyst for ECMO expansion occurred during the COVID-19 pandemic. Hospitals worldwide faced unprecedented surges of patients with refractory hypoxemia. ECMO became a critical final line of defense. The pandemic forced rapid innovation, pushing healthcare systems to expand their ECMO capabilities and driving the demand for more intuitive, portable, and reliable systems. By 2022, the ELSO Registry reached a historic milestone: enrolling its 200,000th ECMO patient and celebrating its 100,000th patient discharged alive [6].
The Modern Era: Understanding ECMO Modalities
Today, ECMO acts as a sophisticated, modified heart-lung bypass machine that can support a patient for days, weeks, or even months [7]. It is not a treatment for the underlying disease, but rather a bridge—providing the heart and lungs time to rest and heal, or serving as a bridge to transplant or destination therapy.
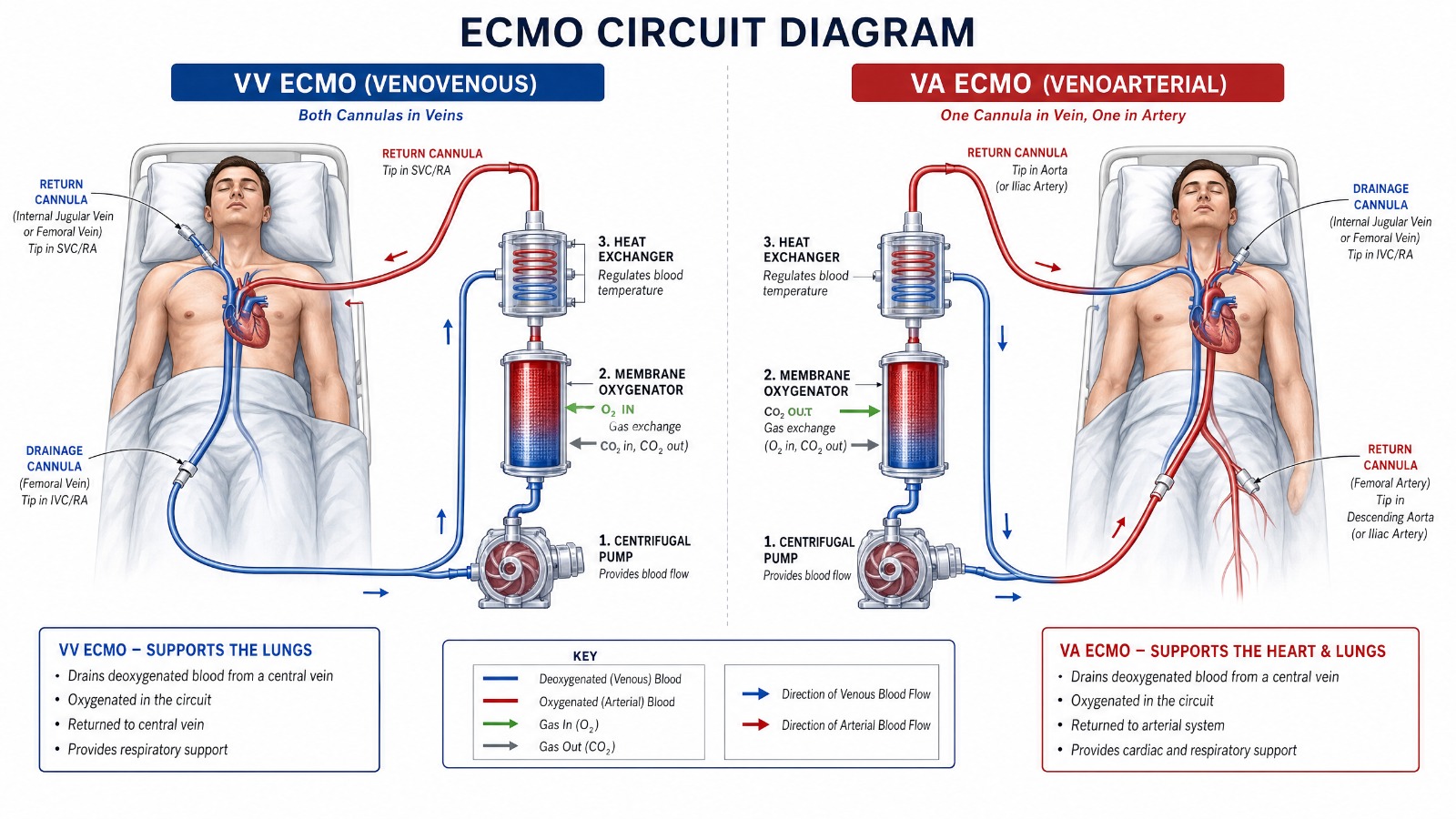
The therapy is generally categorized into two primary modalities:
| Modality | Cannulation Strategy | Primary Support | Clinical Indications |
|---|---|---|---|
| Venovenous (VV) ECMO | Blood is drained from a central vein and returned to a central vein. | Respiratory Support Only. The patient’s heart must function adequately. | Severe ARDS, COVID-19, Pneumonia, Bridge to lung transplant. |
| Venoarterial (VA) ECMO | Blood is drained from a central vein and returned to an arterial system. | Cardiac and Respiratory Support. Bypasses the heart and lungs entirely. | Cardiogenic shock, Cardiac arrest (ECPR), Bridge to heart transplant, High-risk interventions. |
Modern clinical applications continue to push boundaries. As demonstrated by leading specialists, ECMO is increasingly utilized to support high-risk interventions. For instance, ECMO-assisted Transcatheter Aortic Valve Implantation (TAVI) and complex coronary interventions allow physicians to perform life-saving procedures on patients who were previously deemed inoperable due to severe hemodynamic instability [8].
Survival Outcomes and the Importance of Advanced Technology
The success of ECMO therapy relies heavily on patient selection, the expertise of the clinical team, and the reliability of the technology. According to the 2024 ELSO Registry International Report, survival to hospital discharge varies significantly based on the patient population and indication [9].
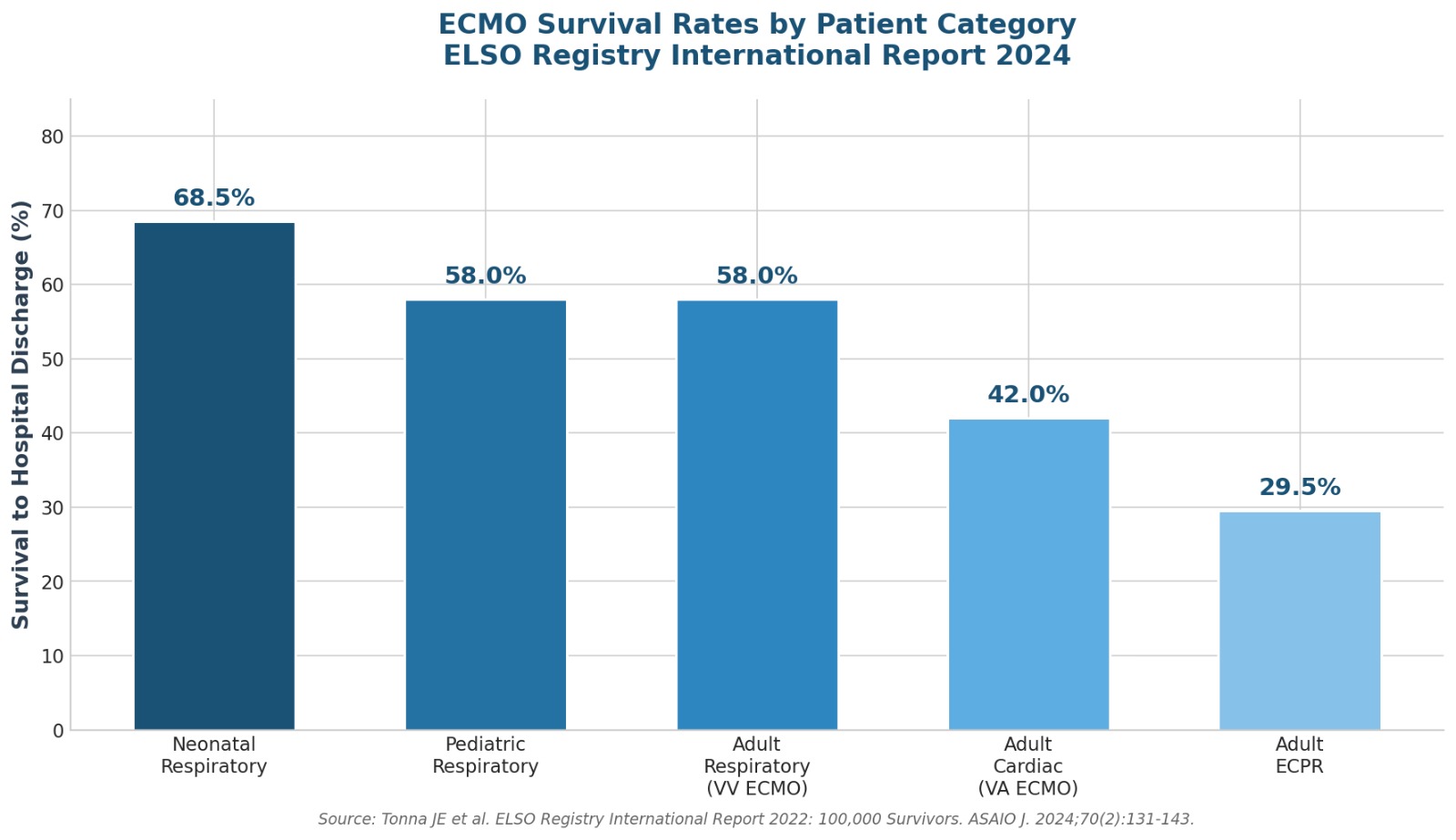
While these statistics represent monumental achievements in critical care, complications such as bleeding, thrombosis, and infection remain persistent challenges [10]. This underscores the urgent need for next-generation ECMO systems designed to mitigate these risks through superior biocompatibility, intelligent monitoring, and enhanced safety features.
Equip your ICU with the highest standard of care.
Partner with
CeroNova
to integrate the Lifemotion® ECMO system into your critical care infrastructure.
The Future is Here: The Lifemotion® ECMO System
As the demand for extracorporeal life support grows across the Middle East and Africa, healthcare providers require technology that is not only highly advanced but also adaptable to diverse clinical environments—from the ICU to emergency transport.
CeroNova is proud to be the regional distributor for the Lifemotion® ECMO System, a revolutionary platform that addresses the historical limitations of older devices. Recently awarded the stringent European Medical Device Regulation (MDR) CE Mark, the Lifemotion® system represents the pinnacle of safety, performance, and reliability [11].

The Lifemotion® Competitive Advantage
- 1 Extended 14-Day Support: The entire system, including its individual components, is certified for sustained critical care use for up to 14 days, providing crucial time for patient stabilization and recovery [12].
- 2 Superior Biocompatibility: The system utilizes advanced Phosphorylcholine coating to significantly decrease inflammation and the risk of thrombosis, alongside PMP hollow fibers for excellent gas transfer and anti-plasma leaking properties.
- 3 Unmatched Portability: Designed for seamless transition between the ICU, emergency department, and patient transport. It features a compact design, a multifunctional trolley, and two independent battery packs supporting up to 240 minutes of continuous operation.
- 4 Intelligent Interface: A high-resolution, detachable display panel integrates real-time monitoring of three pressure sensors, two temperature sensors, and flow/bubble sensors. This eliminates the need for conventional, cumbersome pressure measurement lines.
- 5 Built-in Redundancy: Patient safety is paramount. The system includes a battery-powered emergency backup pump drive, completely eliminating the need for manual hand-cranking during critical situations.
CeroNova: Bridging Global Innovation with Local Expertise
Delivering advanced technology is only the first step. The successful implementation of an ECMO program requires comprehensive support, training, and strategic partnership.

CeroNova stands as the vital bridge between global innovators like Lifemotion and local care teams across the Middle East. We do not merely deliver products; we deliver capability, confidence, and a pathway to hope. Our commitment encompasses the entire lifecycle of the technology—from procurement and installation to rigorous clinical education and ongoing maintenance.
By partnering with CeroNova, healthcare institutions gain access to world-class medical devices backed by over two decades of regional expertise in medical affairs, commercial leadership, and supply chain management.
The evolution of ECMO has brought us from the experimental operating rooms of the 1950s to the sleek, intelligent, and portable systems of today. With the Lifemotion® ECMO system, we are ready to help you write the next chapter in critical care excellence.
Transform your hospital’s critical care capabilities.
Contact the
CeroNova team
today to schedule a consultation and discover how the Lifemotion® ECMO system can elevate your standard of patient care.
References
- [1] Stoney, W. S. (2009). Evolution of cardiopulmonary bypass. Circulation, 119(21), 2844-2853.
- [2] Hill, J. D., O’Brien, T. G., Murray, J. J., et al. (1972). Prolonged extracorporeal oxygenation for acute post-traumatic respiratory failure (shock-lung syndrome). New England Journal of Medicine, 286(12), 629-634.
- [3] Bartlett, R. H., Gazzaniga, A. B., Fong, S. W., et al. (1977). Extracorporeal membrane oxygenator support for cardiopulmonary failure. The Journal of Thoracic and Cardiovascular Surgery, 73(3), 375-386.
- [4] Extracorporeal Life Support Organization (ELSO). (n.d.). What Is ECMO? Retrieved from
https://www.elso.org/extracorporeal-membrane-oxygenation.aspx
- [5] Peek, G. J., Mugford, M., Tiruvoipati, R., et al. (2009). Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. The Lancet, 374(9698), 1351-1363.
- [6] Tonna, J. E., Boonstra, P. S., MacLaren, G., et al. (2024). Extracorporeal Life Support Organization Registry International Report 2022: 100,000 Survivors. ASAIO Journal, 70(2), 131-143.
- [7] Extracorporeal Life Support Organization (ELSO). (n.d.). What Is ECMO? Retrieved from
https://www.elso.org/extracorporeal-membrane-oxygenation.aspx
- [8] ECMO Experts. (n.d.). ECMO Assisted TAVI and Coronary intervention in a High risk Patient Professor Akram Abdelbary. Retrieved from
ECMO Assisted TAVI and Coronary intervention in a High risk Patient Professor Akram Abdelbary
- [9] Tonna, J. E., Boonstra, P. S., MacLaren, G., et al. (2024). Extracorporeal Life Support Organization Registry International Report 2022: 100,000 Survivors. ASAIO Journal, 70(2), 131-143.
- [10] Zakhary, B., Shekar, K., Diaz, R., et al. (2020). Position Paper on Global Extracorporeal Membrane Oxygenation Education and Educational Agenda for the Future. Critical Care Medicine, 48(3), 406-414.
- [11] CBM Lifemotion. (2025). Lifemotion Achieves MDR CE Mark for New Lifemotion ECMO System. Retrieved from
https://www.cbmlifemotion.com/cbm-lifemotion-achieves-mdr-ce-mark-for-new-lifemotion-ecmo-system/
- [12] CBM Lifemotion. (n.d.). Products: Safe Simple Smart. Retrieved from
https://www.cbmlifemotion.com/products/